In November 2020, the mainstay RI team presented at the Symposium on Substance Use Research hosted by the Rural Drug Addiction Research (RDAR), the Center for Biomedical Research Excellence (COBRE) on Opioids and Overdose, and the West Virginia Clinical and Translational Science Institute (WVCTSI).
The symposium provided the mainstay RI team the opportunity to share our work with peers, engage in productive dialogue and feedback, and reflect on our process up until this point.
The original presentation has been re-formatted for this post. The presentation was delivered by Toban Shadlyn via Zoom.
If you missed it: Origin Story (pt.1)

Where the mainstay, RI project is currently
Since the 2019 hackathon win, the team has spent time further developing the project. From our initial research phase and conversations with various stakeholders, three distinct areas emerged for consideration in moving the project from a promising proposal to a more comprehensive plan:
- The Built Environment: the design of spaces (ie. What does a caring environment feel like? How do we design for safety, comfort, zero stigma?)
- Care Team Composition: the support system (perhaps we need to design new kinds of “care teams”)
- Treatment Choice: the many possible pathways to better outcomes (this is often medical treatment but it needs to expand to include housing, cultivating a sense of purpose, repairing relationships, and others. Oftentimes this is predefined, and defined quite narrowly).
One of the insights that came out of these conversations is the limited scientific research on how people who provide or receive care for opioid use perceive elements of that care – in particular the physical environment.

Precedents
As a designer – not bound by the system of scientific research – I look for information, insights, and inspiration all around me. These sources of learning can be closely related to the topic as well as analogous to it, often in unique or unexpected places/spaces.
For example, we are looking at exhibition design (temporary and mobile characteristics) to adapting existing infrastructure (permanent yet flexible) as we consider the potential for care and harm reduction in our built environment and physical spaces.
Pictured above:
- CODAC’s mobile health clinic: moves around to different neighborhoods across the state of Rhode Island
- The ‘Engagement Center’ in Boston: a temporary tent in a parking lot for people who are homeless to visit during the day, receive services, and connect with their community
- SAFE SHAPE: a ‘pop-up’ traveling exhibit in the form of a pavilion that operates as a mock drug consumption room (DCR). DCR’s, also sometimes referred to as Safe Consumption Sites, are not yet legal in the US. This is perhaps a creative roundabout way to still prototype something and solicit feedback from the public, while current challenges of legal barriers still loom.
- Wyndham hotel in Warwick RI: during COVID, they adapted their facilities to house people who are homeless and frontline care workers. Interventions like this, enable us to ask questions that maybe would have been “too far-fetched” to ask pre-COVID like: “How can we adapt existing architecture and spaces to provide harm reduction and recovery services?” (hotels, community centers, churches).
Though these precedents are helpful to a certain point, it is critical to understand the cultural context in which we are operating. What works in say a city like Vancouver Canada may not succeed if copy and pasted into Providence Rhode Island. These two places are very different from one another, with their own unique set of challenges specific to the context in which they are situated. However, understanding the key design principles that have led to successful societal outcomes can perhaps be transferred across different contexts.
Visuals
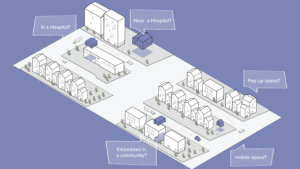
We have created visuals and sketches as a tool for engaging with one another and with external collaborators. These visuals are not intended to depict the solution, but rather a tool for asking questions, prompting conversations, and creating shared visions of what could/should be (provocations of a preferred future).
As an example we created the visual above to spark a conversation around the different possibilities of mainstay, RI as a place and/or space: “Is mainstay a room or in a wing of a hospital? Is it near the hospital, or embedded in the community? Does it move around from neighborhood to neighborhood? How flexible or permanent is the place, does it pop up and pop down?” Is it a combination of all of the above…?!
These questions and visuals help us not only confront the practicalities and specifics but open up space to engage in conversations that radically reimagine how we understand and design for “care”. Does care for substance use require the presence of medical support? What would it look like to design care around connection?
IRB Research & Interviews
Currently, we are in the process of conducting interviews with people who use opioids and have experienced an overdose, as well as those who care for people who have overdosed (nurses, friends, peer recovery coaches). Due to the nature and sensitivity of this topic, it was important for our team to obtain IRB (Institutional Review Board) approval, to engage with this particular group while ensuring their protection and confidentiality. These conversations are intended to surface insights around the 3 focus areas: care team composition, care treatment, and care spaces.
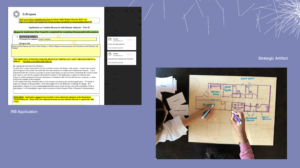
The image on the left is a screenshot of our IRB application (likely familiar to all the scientists reading this). But for our team, some of us are learning to navigate the IRB system for the very first time. While others on our team are learning about some of the informal and interactive ways designers might engage with people. The image on the right is a prototype of an engagement tool for sketching people’s experiences in care spaces and how they would redesign a space for care.
These tools are important to show in tandem. We are interested in creating conditions and relationships that aren’t limited to the transfer of information but can enable co-creation. Providing people the tools (in this case a whiteboard and pen) to communicate, collaborate, and design.

Where the project is going
While IRB interviews are underway (we will be sharing the insights from those conversations in the coming months), we have also been speaking with other folks across the problem space (ie. law enforcement, community-based organizations, etc.), learning from their unique perspectives to help inform the project. Some initial themes are:
* Provider fatigue amongst:
- Health care providers (there is a shortage of bilingual care professionals in Rhode Island)
- Police administering naloxone daily (secondary trauma and fatigue)
- Family members providing ongoing support
* The urgency and need for different kinds of housing support
* The rapidly changing landscape of treatment (due in large part to COVID-19)
Many of these insights are not surprising but are important to surface as they reveal information that is unique to the Rhode Island context.
As we head into Spring 2021, the team will be wrapping up our IRB research and interviews which will close out our current grant funding. We will spend some time reflecting on our learnings over the past year and strategizing the next steps for the project. Stay tuned for part 3!
Visit the website to read more: mainstayri.org
– Written by Toban Shadlyn. March 2021.