Reimagining the Purpose and Efficacy of Morbidity and Mortality Conferences (M&Ms)
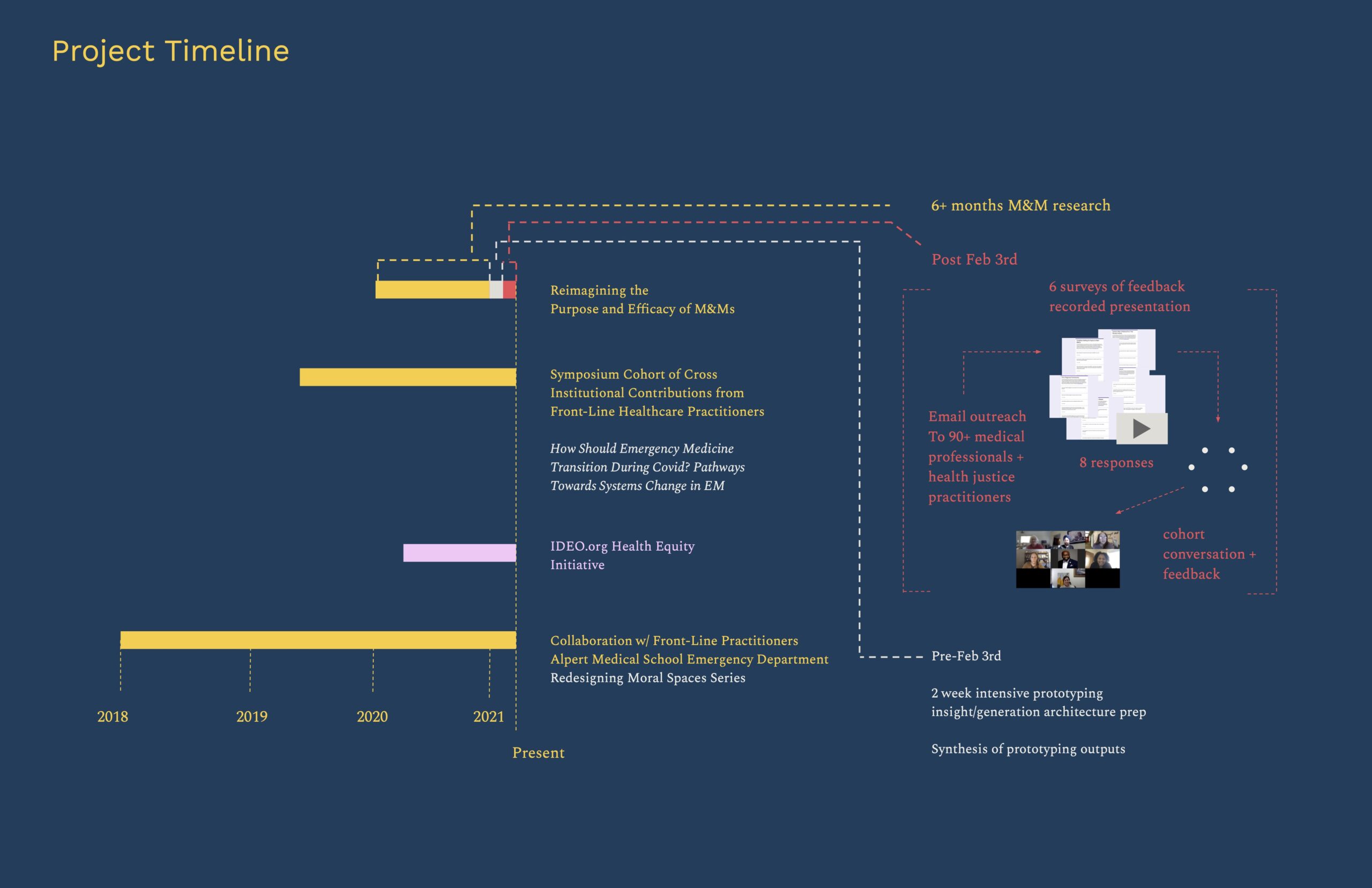
What follows are slides and accompanying talking points* presented by CfC leads Julie Woods and Sahib Singh during a 03.10.21 gathering of the Health Equity Collective (HEC). The HEC is funded by Robert Wood Johnson Foundation and CfC has been a member since its start in summer 2020. This slide deck synthesizes the value and opportunity in the redesign of the Morbidity and Mortality Conference (M&M) and the 6 interventions designed by CfC to achieve improvement: The Framing Studio on Morbidity and Mortality Conferences; Prototypes for Reimagining the Morbidity & Mortality Conference (M&M)
*with some updates
This project focuses on redesigning the Morbidity and Mortality Conference (M&M) –
The M&M is a medical forum with over 100 years of tradition that provides clinicians the opportunity to review and discuss adverse events and medical errors.
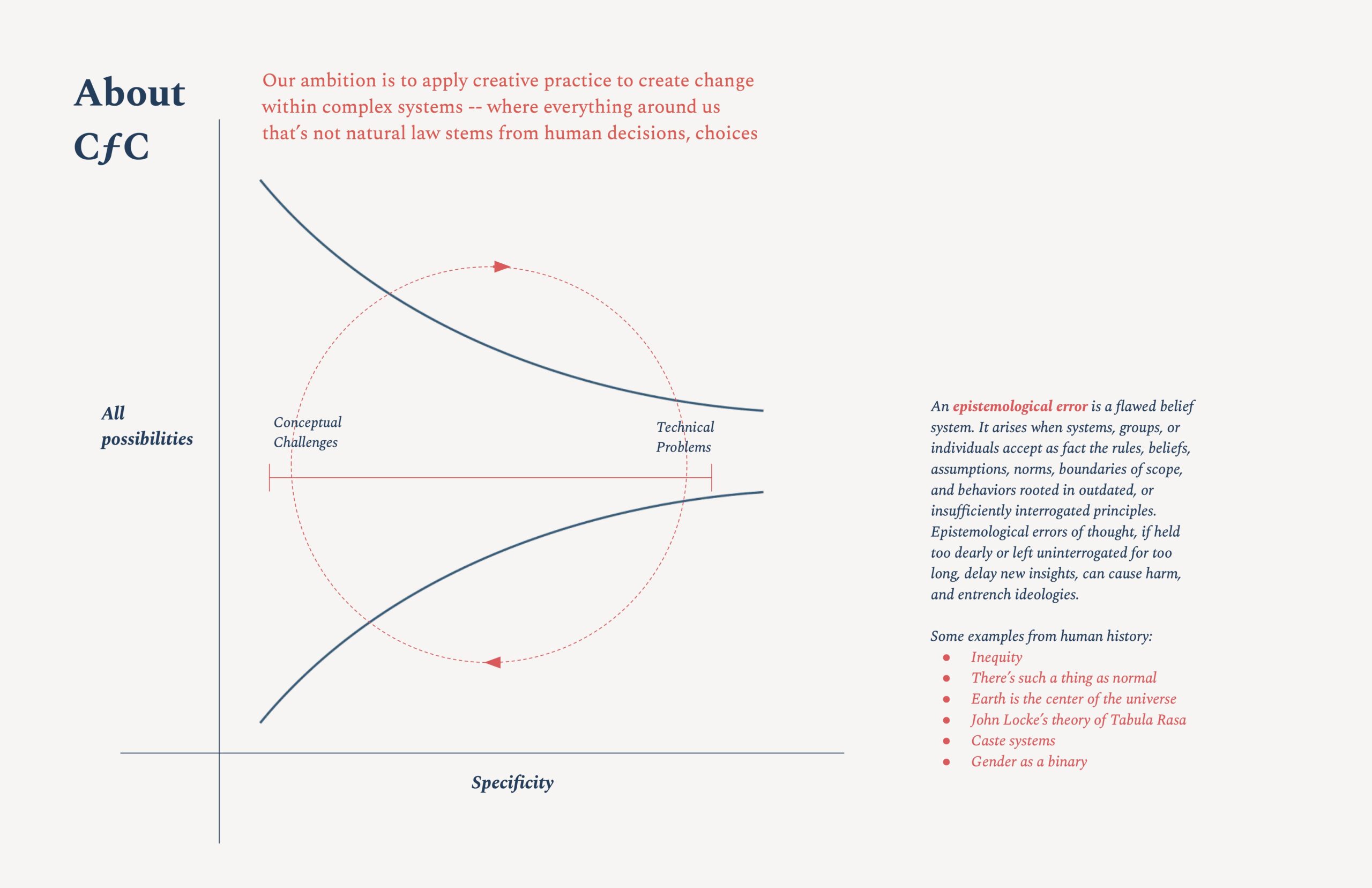
CfC believes that the redesign of the M&M could be the core of an ecosystem of interventions for reducing adverse outcomes.
For over 100 years, M&Ms have been a space to provide accountability and opportunities for education in medical practice.
Despite these stated goals and long tradition, medical errors are widely reported to be the 3rd leading cause of death in the US. (Two years after this presentation, medical errors continue to rise, perhaps exacerbated by staffing shortages and other repercussions of the global pandemic: Joint Commission Sentinel Event Data Summary. )
Is the M&M an artifact or anachronism? Is it a vestigial appendage? No – it is an opportunity. Rather than build a completely new system for investigating and addressing adverse events, the M&M, a staple of learning and improvement, can be modified.
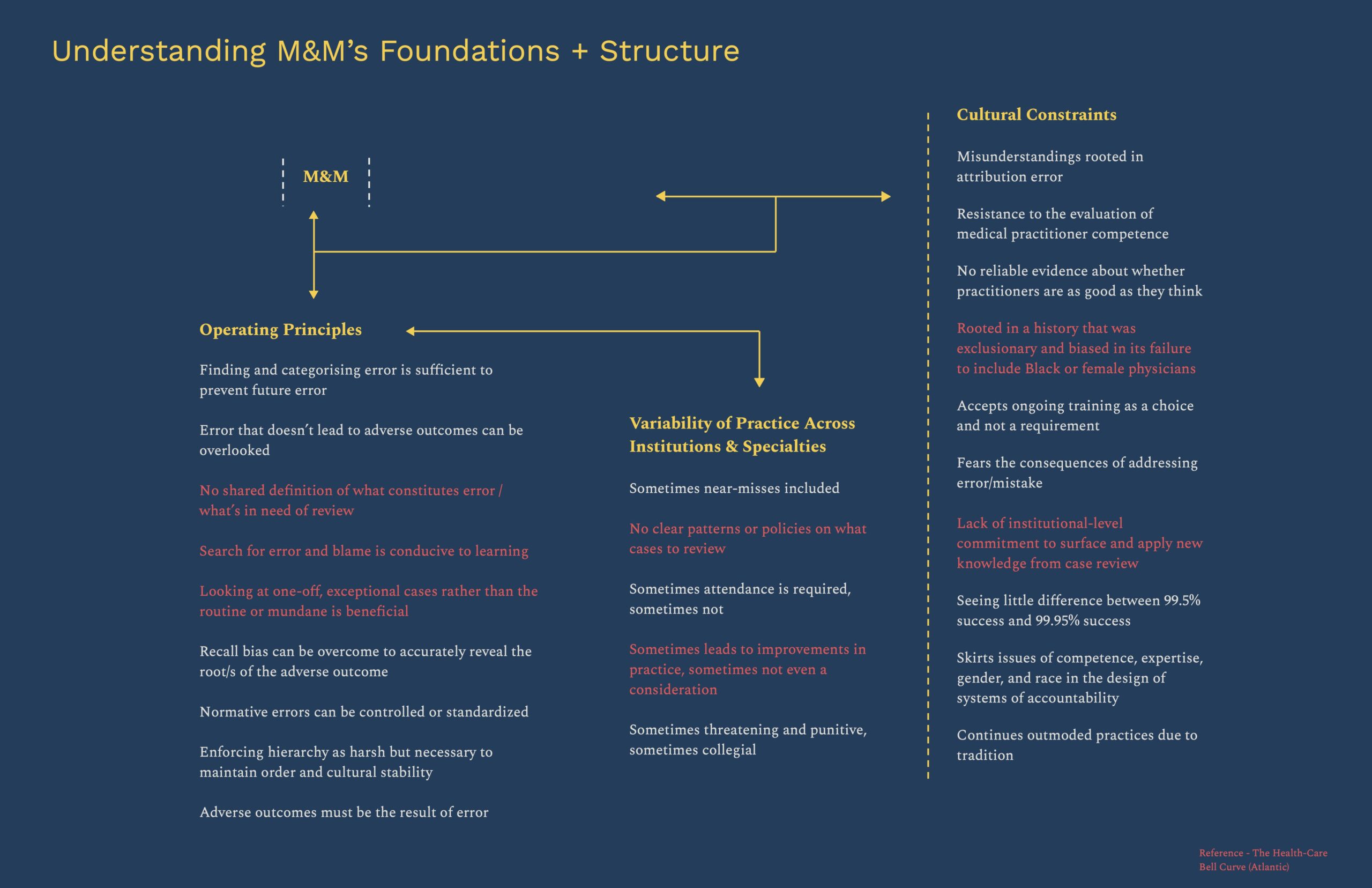
M&Ms take place across all medical practices and specialities, but are highly variable, built on a culture of fear and control, a focus on error and mistake, and largely unchanged over its history (Bosk)
Our research suggests that there is:
no shared definition of what constitutes error
no agreement on what’s in need of review
no questioning whether the search for error and blame is actually conducive to learning
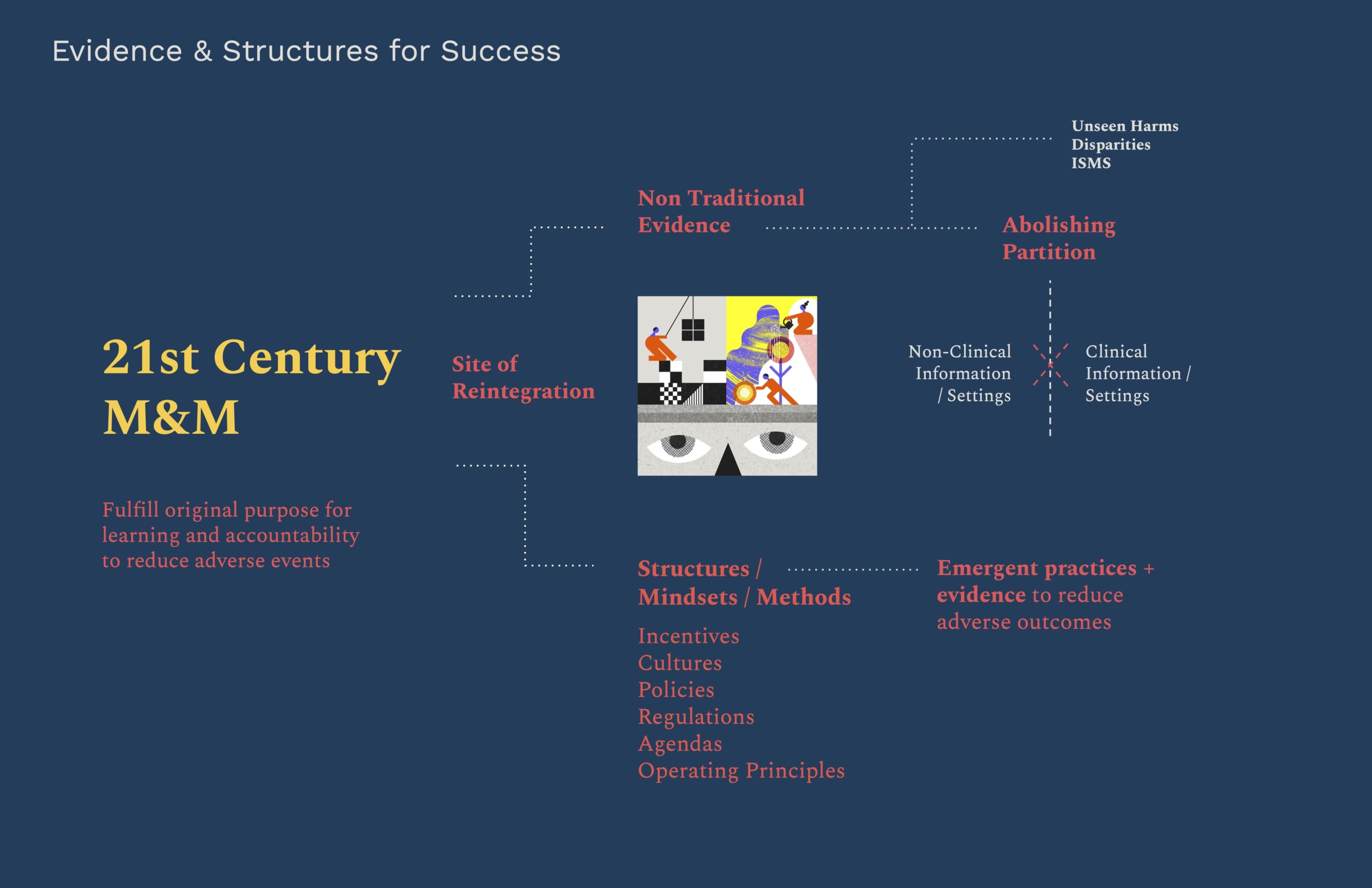
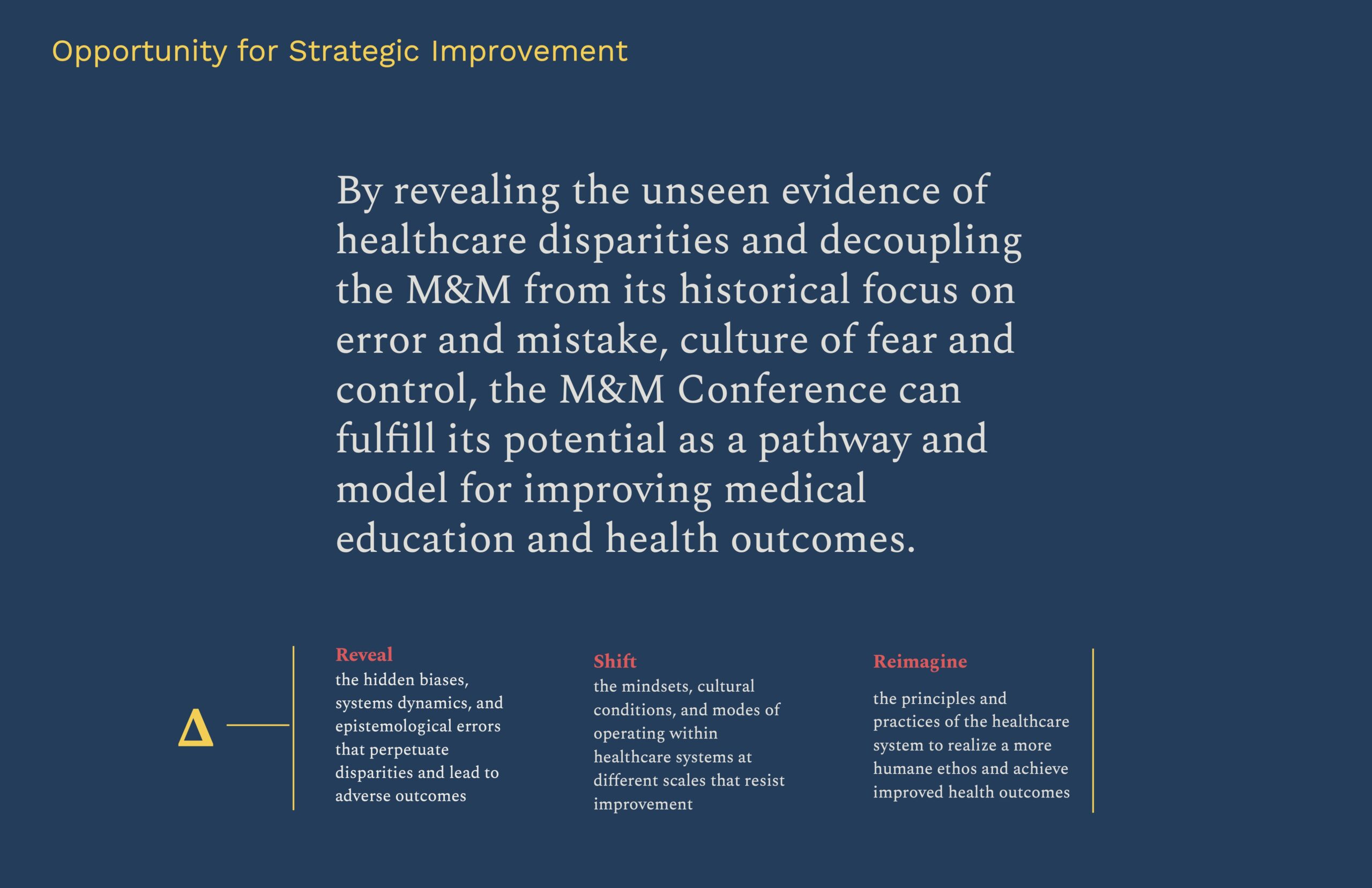
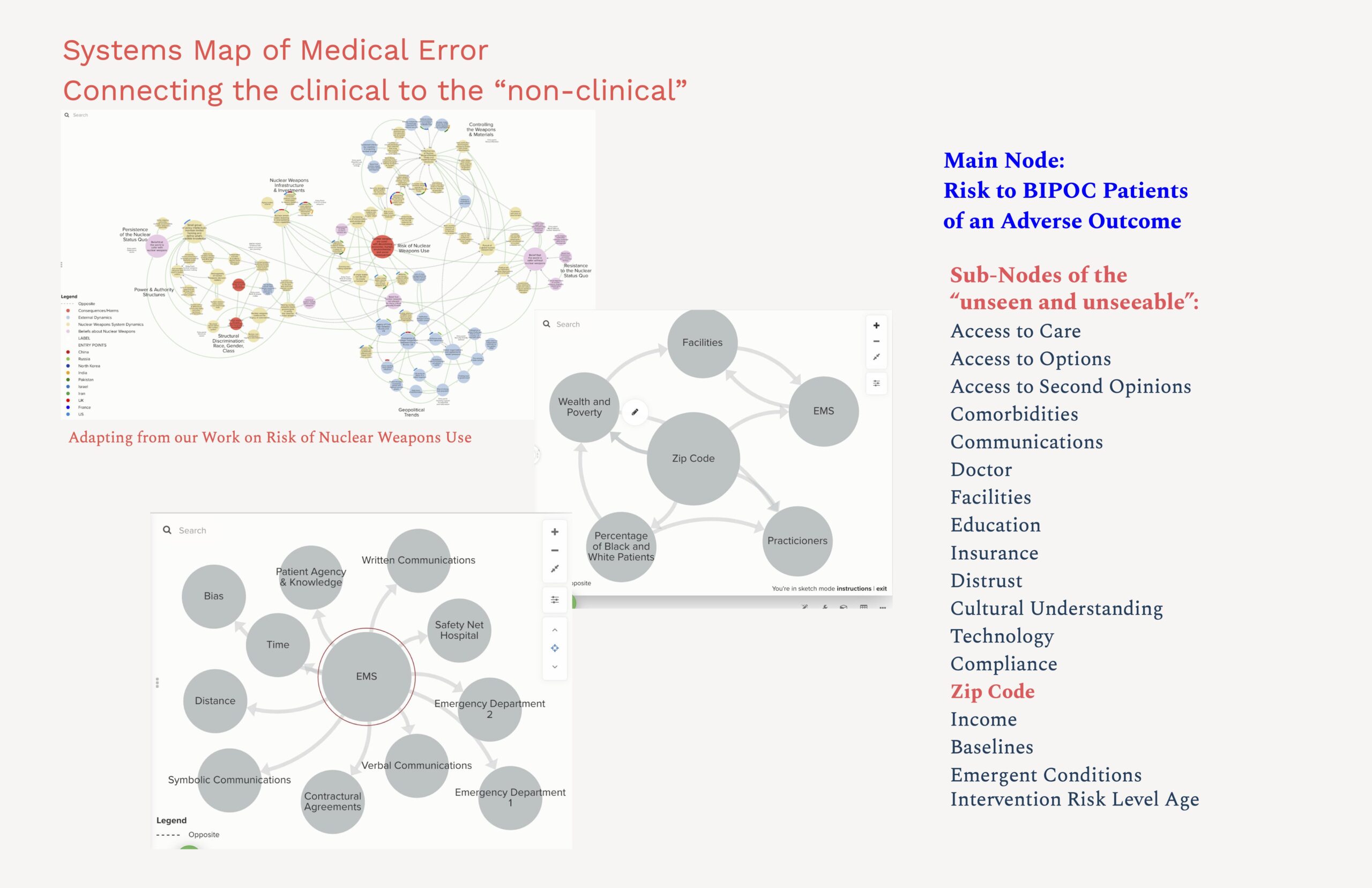
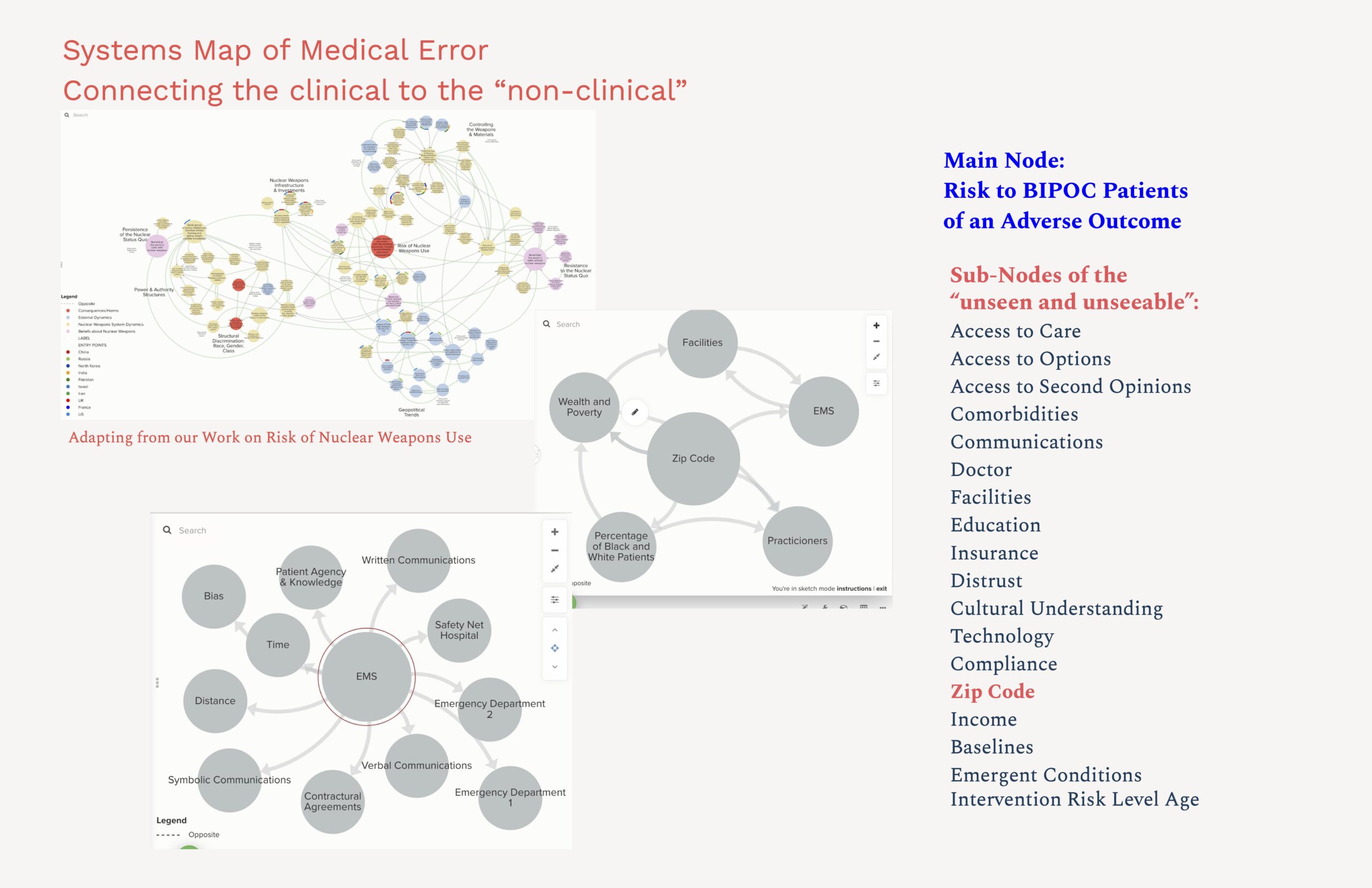
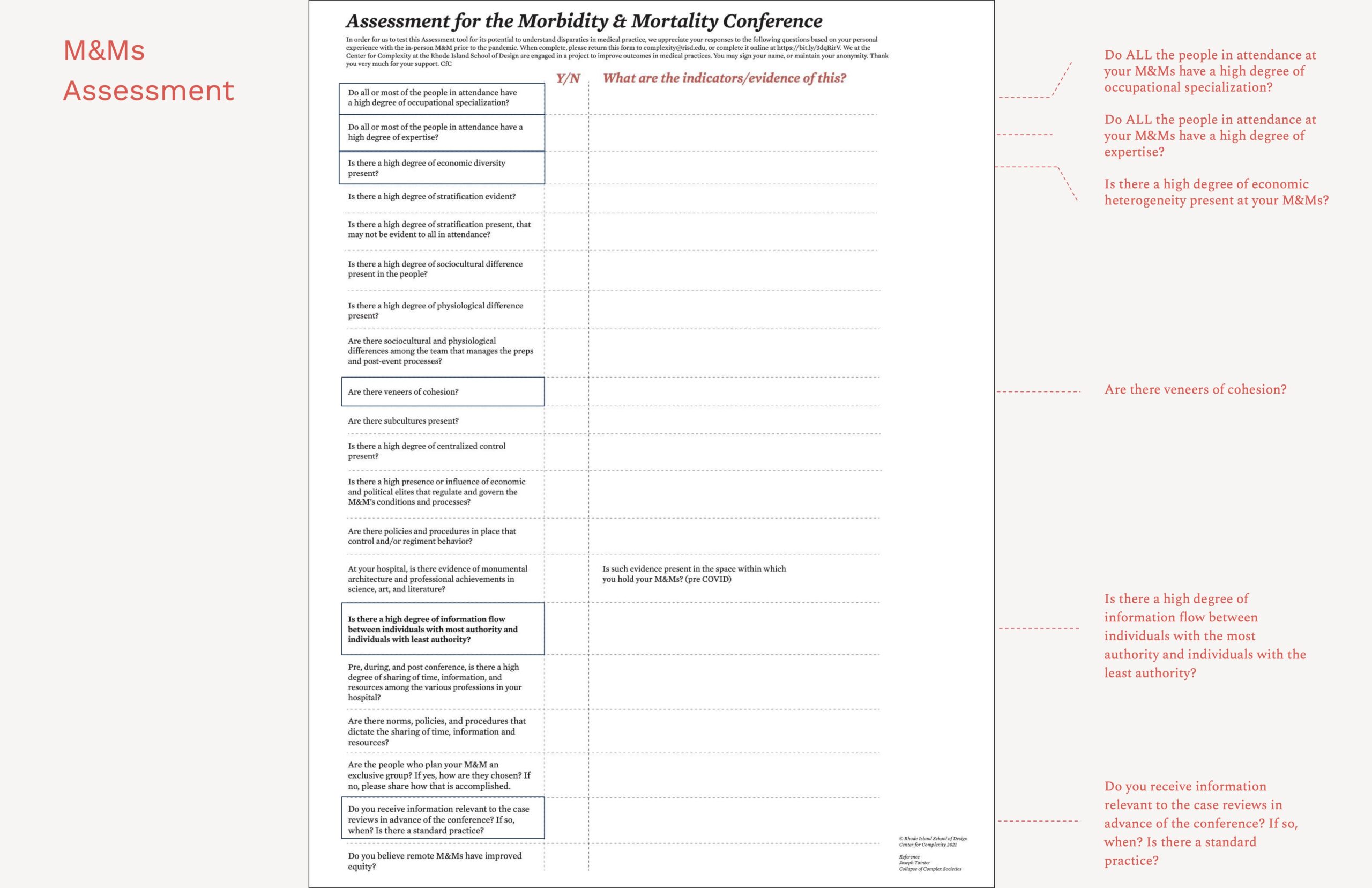
The current limitations can be overcome and the M&M can be a site of integration of non-traditional evidence and new feedback loops to advance emergent practices.
- By taking in new sources of information and evidence currently excluded (abolishing the partition between what’s clinical and non-clinical–seen at top right of the slide) and by making visible the unseen – and undocumented) instances of poor outcomes and harm.
- By creating feedback loops to disseminate and integrate new kinds of evidence and emergent practices to reduce adverse outcomes.
A 21st century M&M requires new structures, mindsets and methods necessary to successfully reach out – not just to allies and would-be allies – but to those in power who could resist improvement.
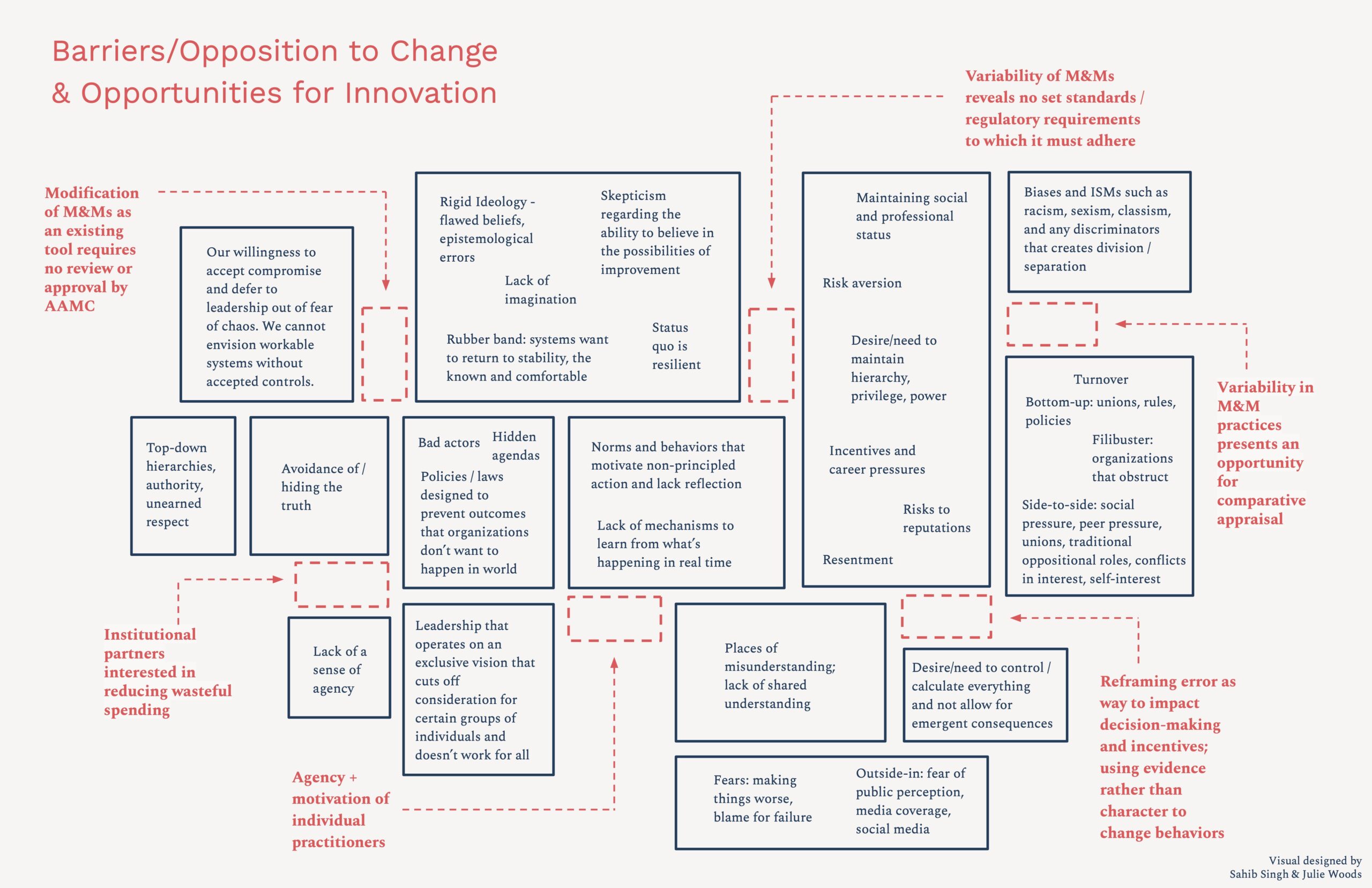
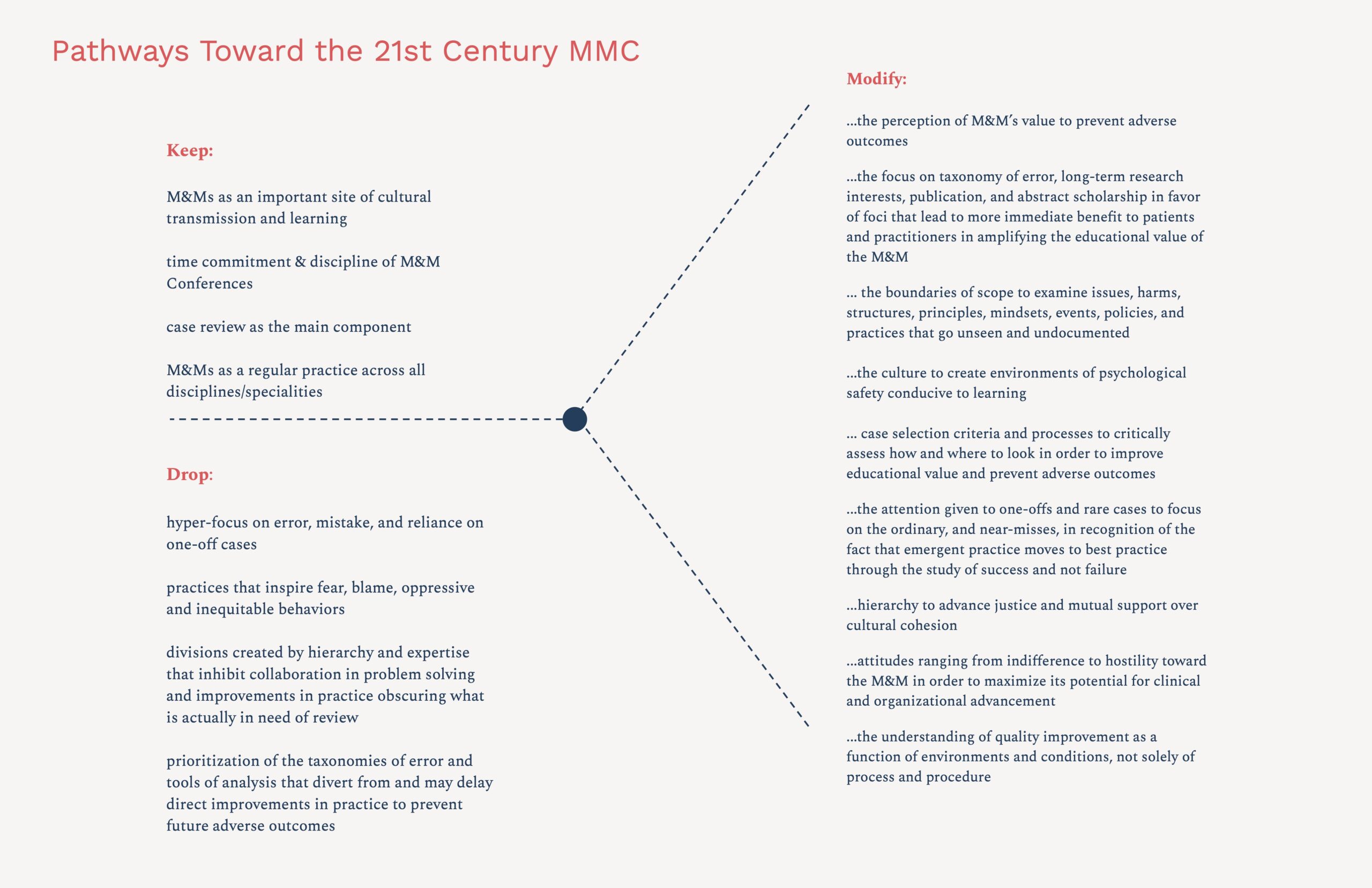
In all systems redesign it’s wise to anticipate resistances to change. What you see here in dark blue boxes are common barriers to achieving sustainable change. All systems want to revert to the known – like a rubber band. Barriers can be recast as opportunities using a tool such as the graphic above – called out here as red dotted boxes.
2 opportunities to highlight –
- The M&M doesn’t require review or approval by AAMC – it’s not the introduction of a new system of medical education
- The variability across M&Ms and lack of set standards or regulatory requirements means that experimentation is possible.
Our feedback sessions with medical professionals and health practitioners pointed out that in addition to benign sources of resistance there’s direct opposition to disparities that must be confronted.

A key insight from health practitioner feedback is the need to use different vocabulary when communicating with different groups. Error, rather than equity, for example, is the vocabulary of risk and insurance.
This insight helps us reach out to would-be allies for whom financial considerations – and not disparities – are a priority. In this way new alliances can be built where the goals can be the same though the motivations may be very different.
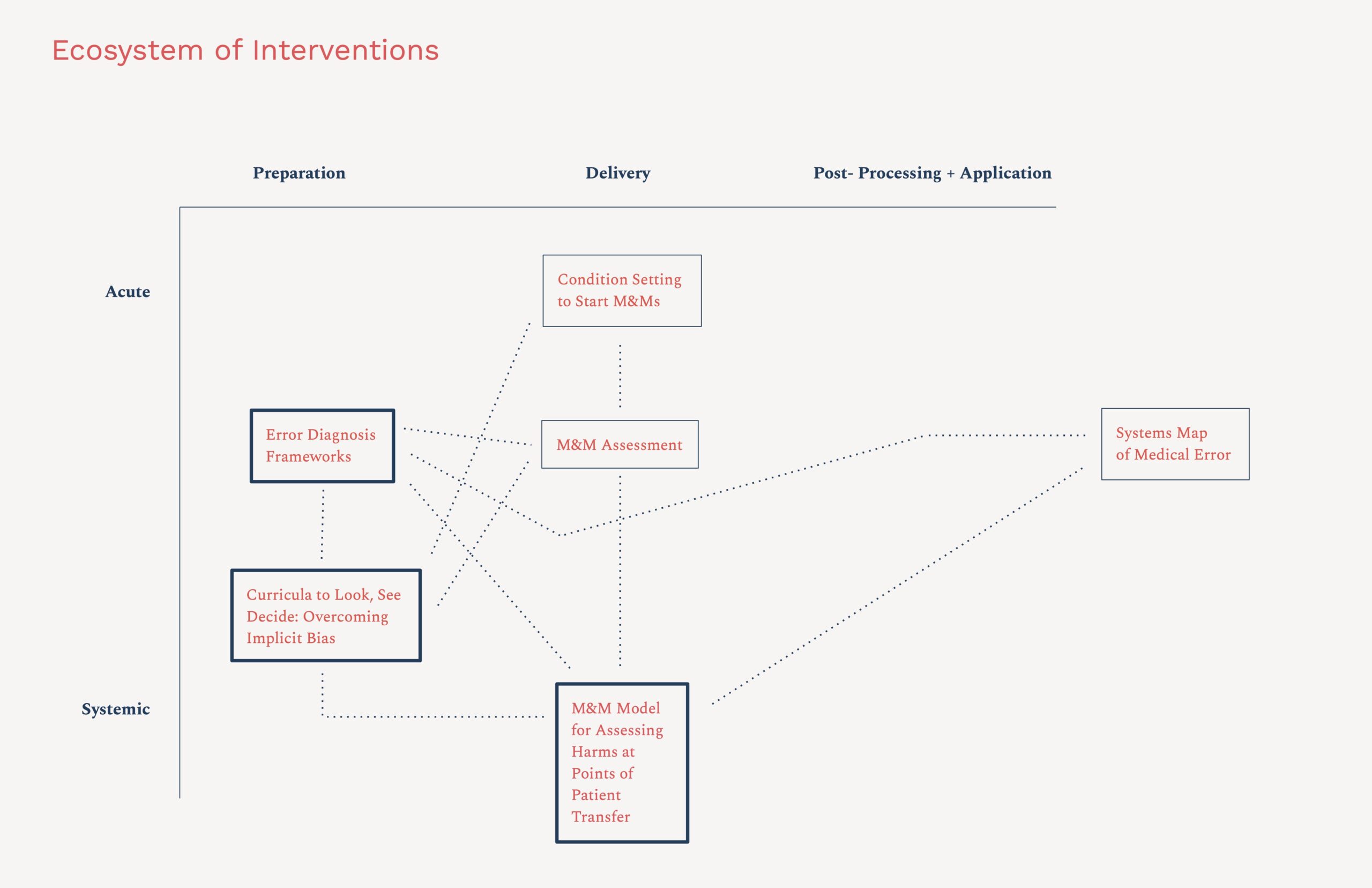
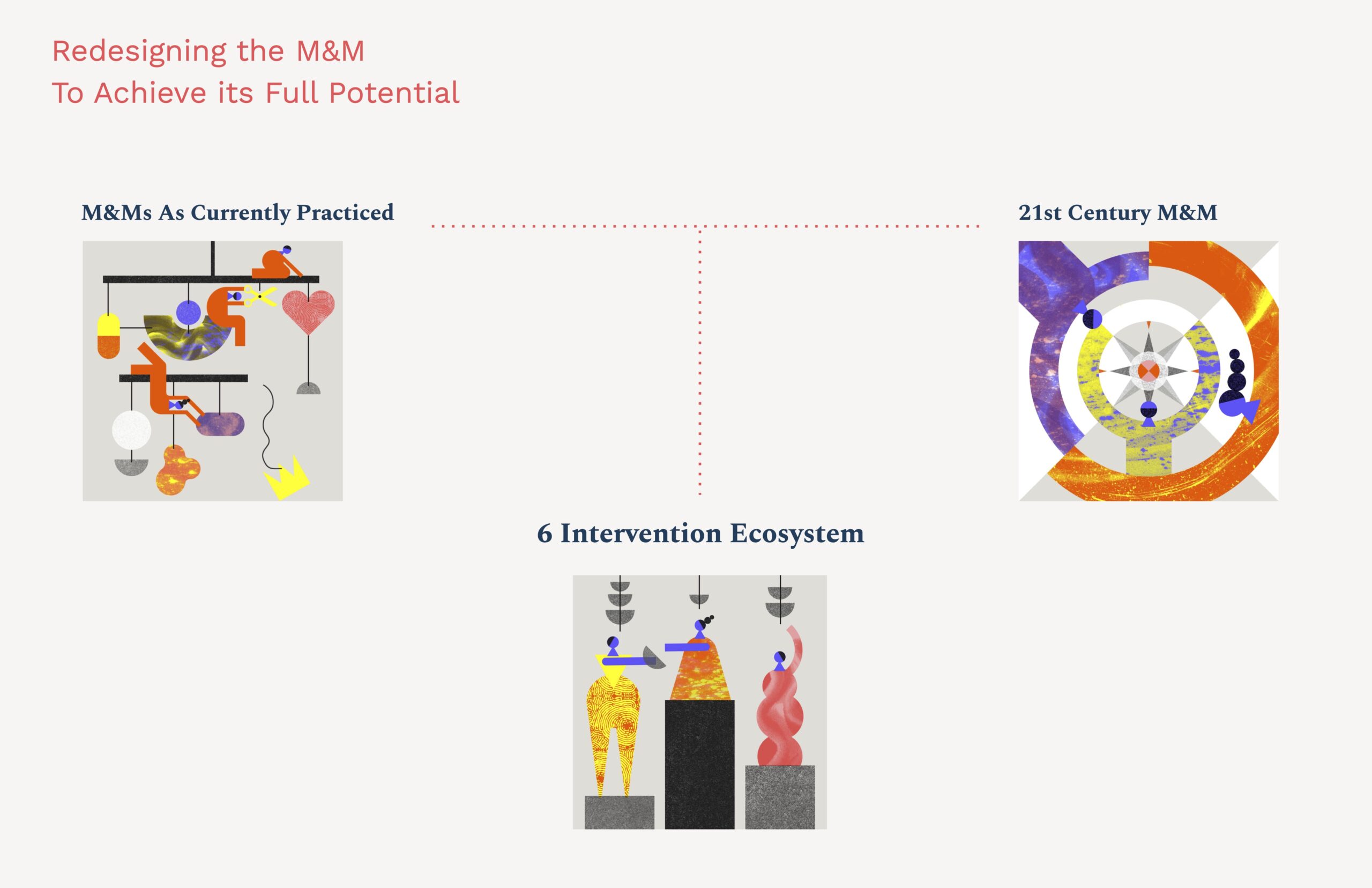
We must employ many pathways to get to a 21st Century M&M. A complex system requires a complex response. An ecosystem of interventions is needed to achieve systems improvement -, working together at different scales and applied at different points in the preparation, delivery, and outputs of the M&M.
For the purposes of this short presentation we will focus on three of the 6 interventions we have designed. These 3 emerged as most popular among our clinical colleagues, based on feedback received through email, meetings, and surveys. These interventions operate at different scales and work at different entry points to shift the mindsets of practitioners in the M&M and the structure of the M&M itself.
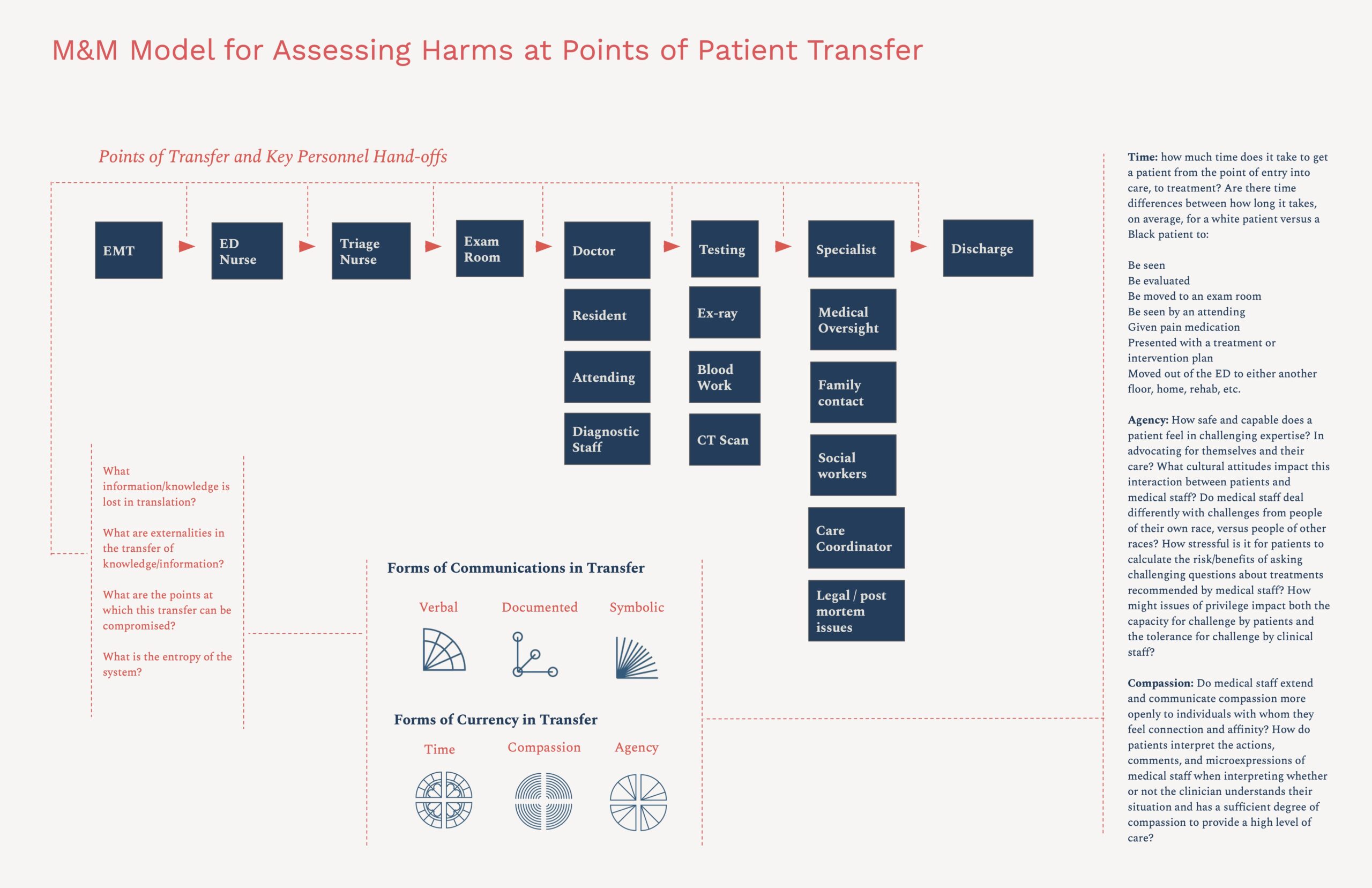
M&M Model for Assessing Harms at Points of Patient Transfer — are a non-hierarchical, cooperative model that would bring together professionals from across the patient handoff process — illustrated here.
M&M Model for Assessing Harms at Points of Patient Transfer would apply the insight and knowledge of professionals throughout the patient experience, identify the information lost or compromised in transfer and translation, and incorporate evidence not currently considered pertinent in the consideration of conditions that lead to adverse outcomes.
M&M Model for Assessing Harms at Points of Patient Transfer would examine the three traditional forms of communication – verbal, documented and symbolic, as well as any discrepancies in the distribution of what CfC defines as the three currencies of the healthcare environment: time, compassion, and patient agency.
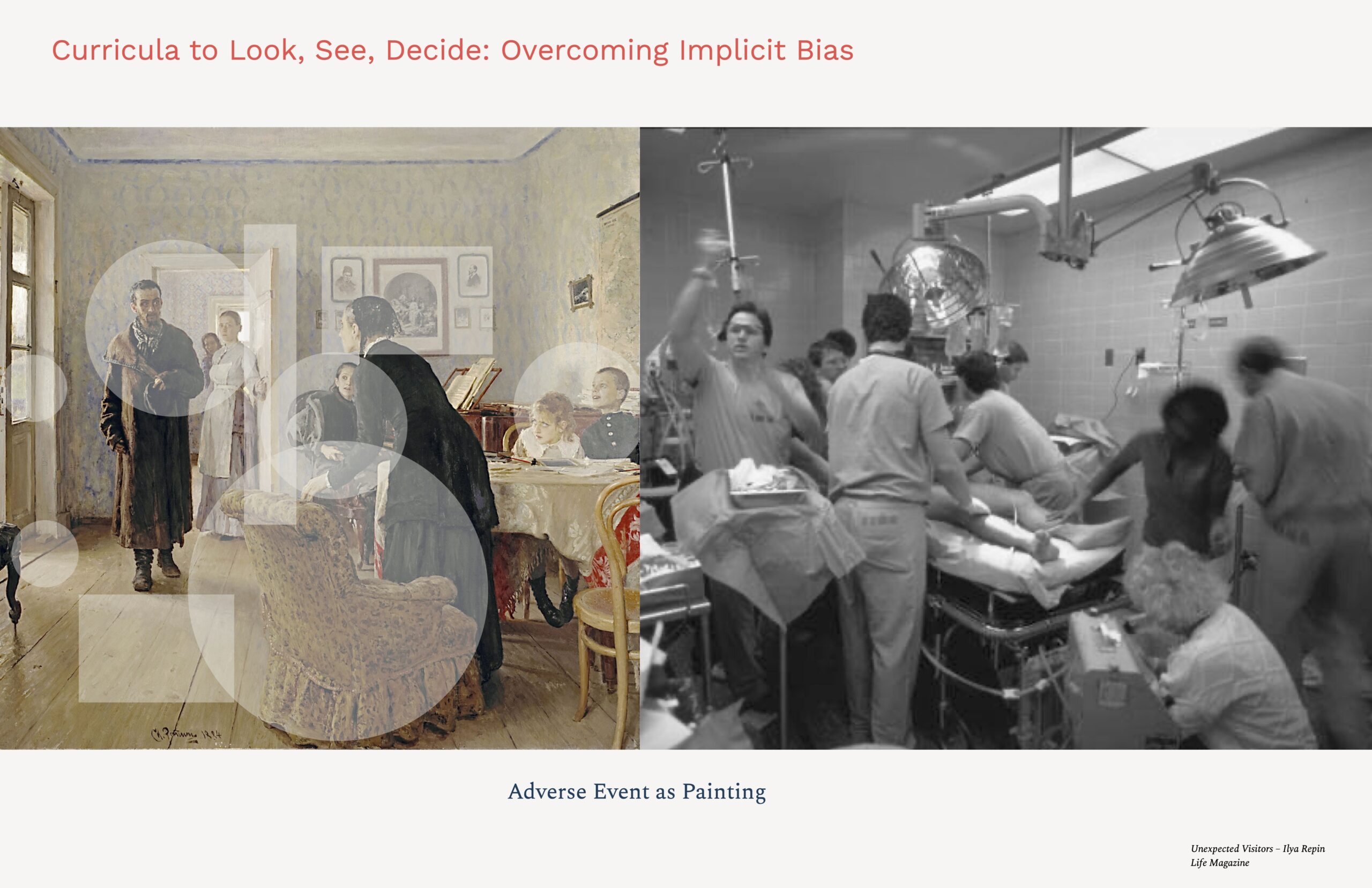
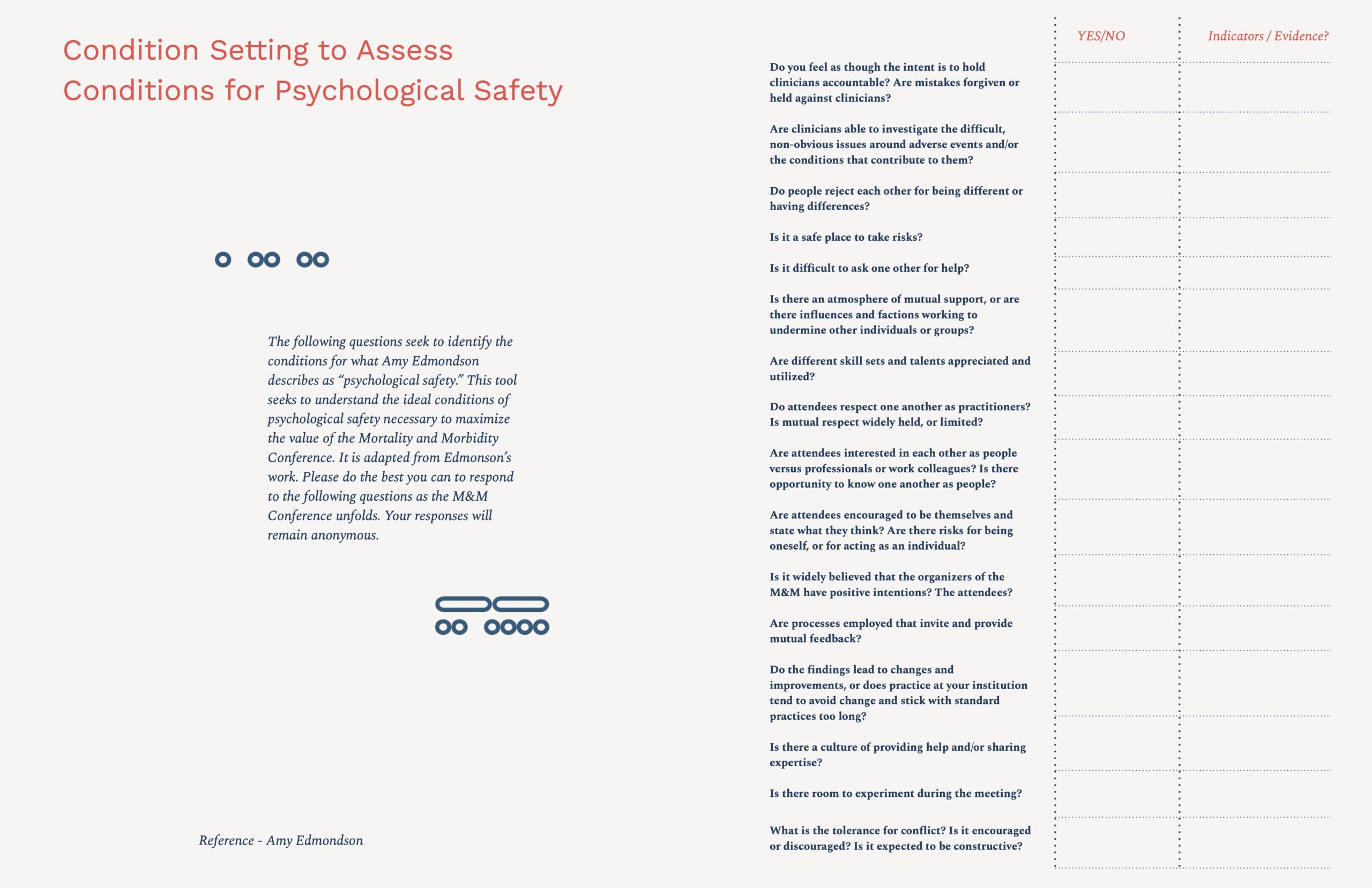
Curricula to look, see decide – employs visual art to surface and destigmatize implicit bias, yielding new evidence to understand the variations in how individuals respond to visual information, how we automatically make determinations about what visual information is relevant and irrelevant, and how this automatic process impacts the inferences we draw and the decisions we make. The human brain “takes only 13 milliseconds …to process an image.” Learning to pause and reflect or to question our initial assumptions may be required in order to avoid actions and decision-making that lead to adverse outcomes.
Cognitive biases influence how, where and why we look as we make sense of the circumstances around us, wired into us by evolution, culture and experiences. Discussions around bias need not be accusatory but can be generative and lead to individual and team insight and growth.
When we look at The Unexpected Visitors painting by Ilya Repin, we might ask
Who is this woman in black in the foreground?
The person waiting in the hallway?
Are people shocked, angry or happy at the arrival of the visitors?
What are the relationships between and among the people in the painting?
Similar questions arise in real-world situations.
The scene in the ER to the right is like a painting. We as viewers make sense of what we see. But, as we enter this ER setting, which visual information is most relevant as we determine what is happening and where to focus our attention and action first?
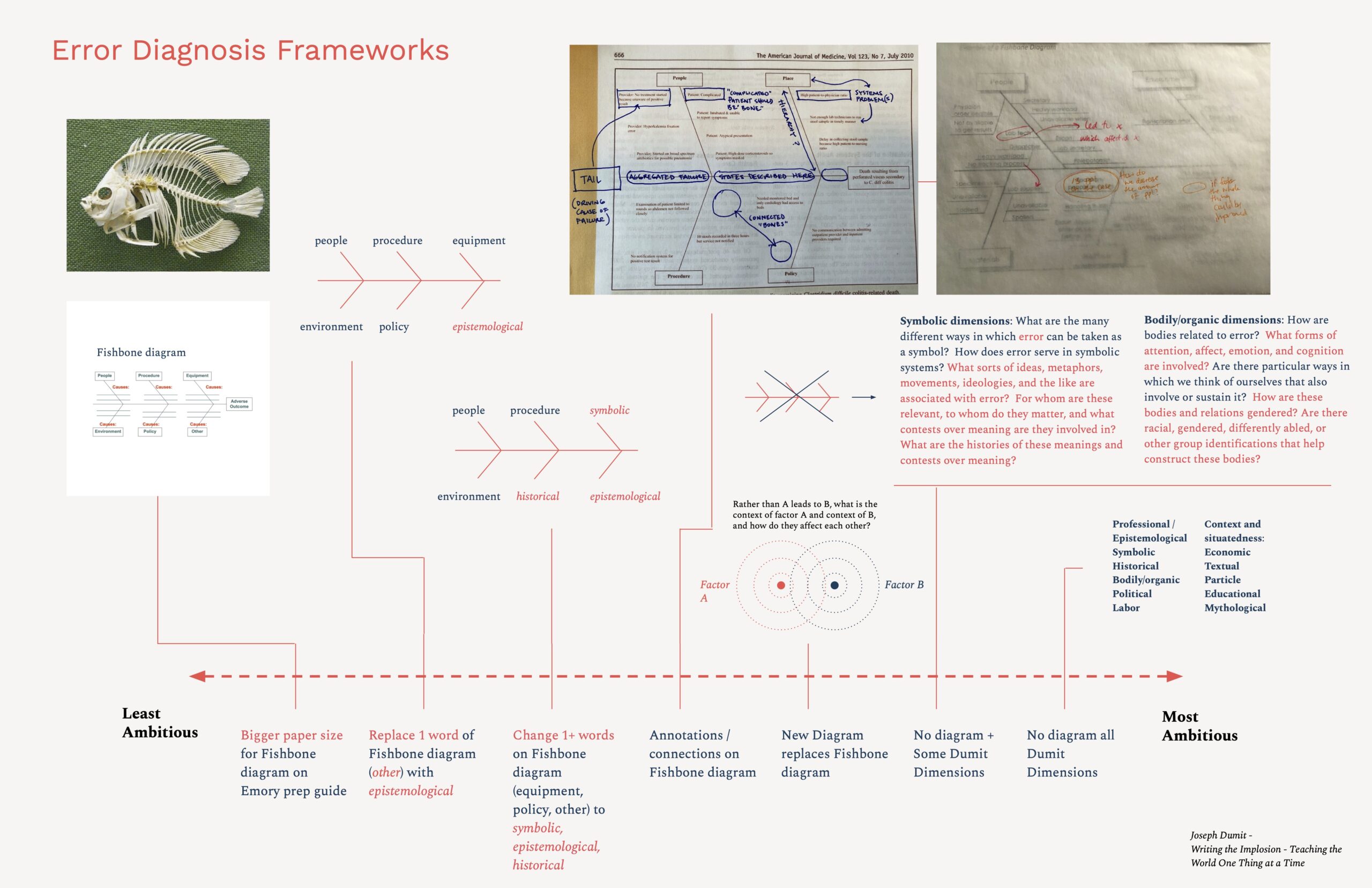
Error diagnosis frameworks are redesigns of the tools of analysis (heuristics, diagrams, etc.) which potentially limit where and how clinicians look to evaluate the causes of adverse events.
One popular tool adopted from a manufacturing model developed in the 1960s is the fishbone diagram used for determining root causes. Adapted from manufacturing — is it suitable? Is it too reductive? Do such tools hide/crowd out complexity? Is root cause even an adequate framing to understand what could be relevant to an adverse event? Sixty years on, this tool and others like it may present an opportunity for redesign that embraces the complexity of decision-making, including a consideration of bias that’s currently left out of consideration in analysis.
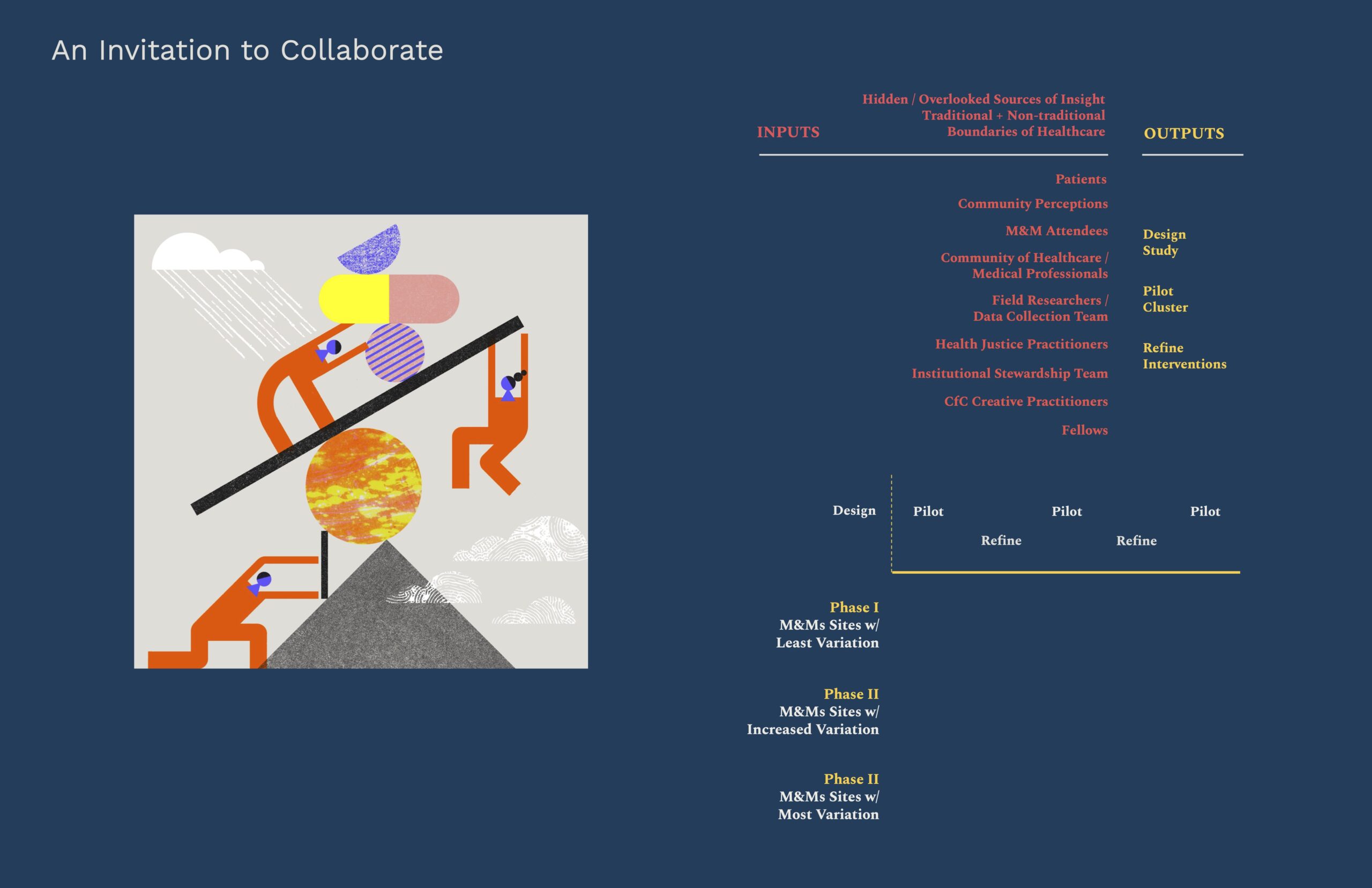
To successfully yield new insights, this project will have to take input from a wide range of stakeholders and community members, including voices from outside the traditional areas of consideration and centering the knowledge and experience of patients.
To achieve greatest impact CfC will design an applied research process, gathering those inputs and synthesizing those learnings to identify relevant research questions, and designing processes to:
- develop interventions which would seek to shift mindsets and courses of action within the delivery of care
- test the efficacy of our interventions through piloting at various sites and;
- achieve and promote learnings and additional interventions that could reduce adverse outcomes at and beyond the prototyping sites.
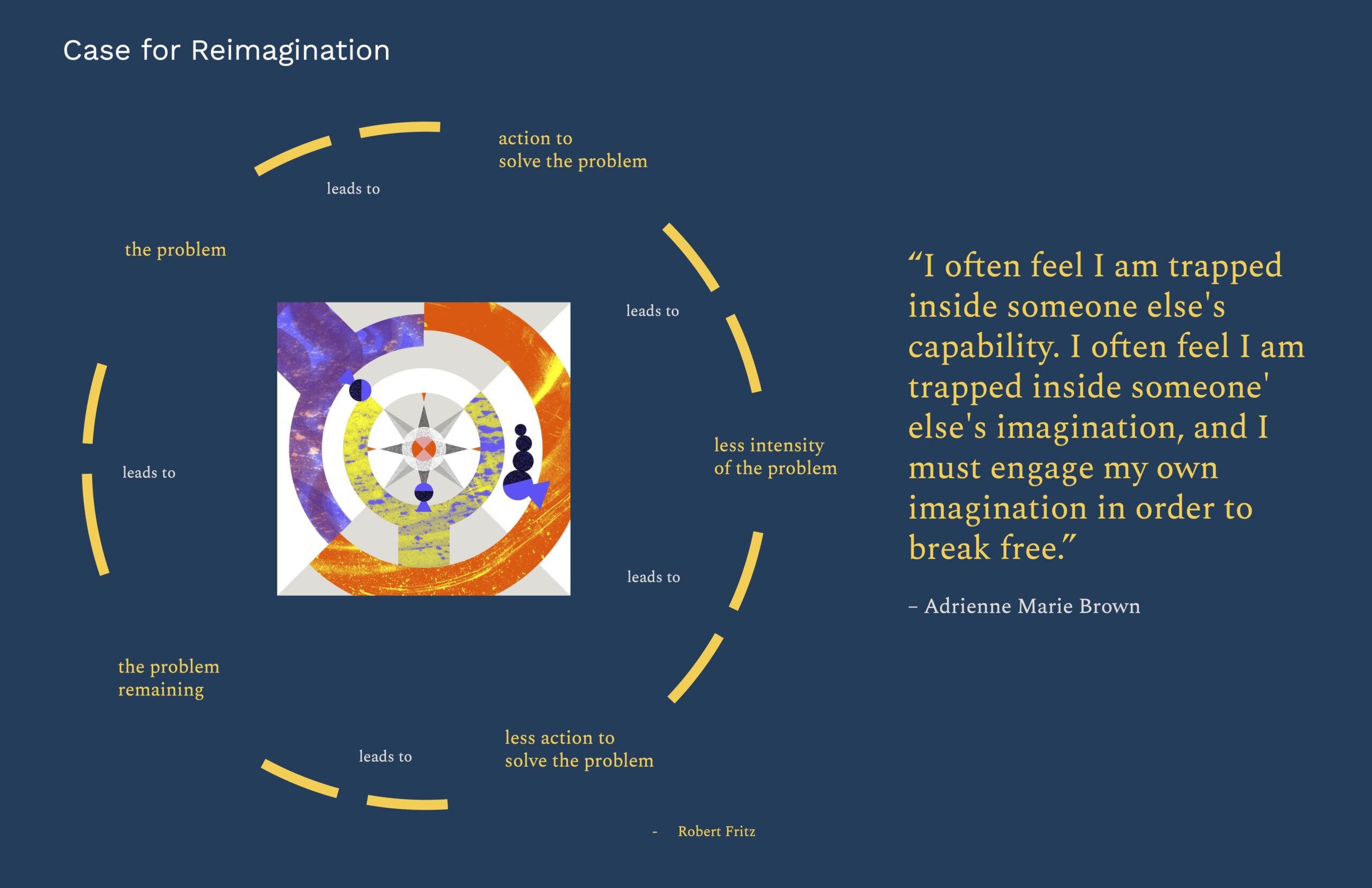
21st Century M&Ms require breaking free from a problem solving cycle that is trapped in traditions that no longer serve medical practitioners nor the purpose for which M&Ms were created: to review and learn in order to reduce adverse outcomes.
It requires breaking free from the limits of its history and past practice.
Taking inspiration from Adrienne Marie Brown, we need to apply imagination to break free from systems that trap us in other peoples’ imaginations in order to improve health outcomes.
We’re grateful to all of you.
We intend to carry this work forward and hope to activate future collaborators from among this amazing community.
Thank you.
Oh an there’s an appendix if you’re interested